
6 Common Positioning Frustrations That Mammography Technologists Encounter
- You need to be doing “perfect” ACR images on every patient.
- You must do additional views every time there is a skin or fat fold.
- You need to visualize pec muscle on every CC.
- If the IMF is not visualized as open and without folds, an additional view should be done.
- Do XCCLs on all patients that have posterior breast tissue going off the lateral edge of the CC.
- You need to do 10 images for all patients with implants.
Studying Common Positioning Problems
Did you know there is published data on most of these “repeatable” offenses? AJR (American Journal of Roentgenology), with the help of our lead educator, Louise Miller, published an article that most of your radiologists should probably read.
The research team, along with Ms. Miller, measured each characteristic of hundreds of CCs and MLOs. They also made sure the technologists had been trained using The Miller Method™ of mammography positioning, which combines both the ACR method and a bit of the Tabar, or Swedish mode, a method we used because the Swedish technique has proved to be super efficient and ergonomically sound.
After doing a positioning training for all technologists with FFDM (which was different from Film Screen), we then had a follow up training after the installation of DBT (which was different from FFDM).
When we compared our scores to those shown in a paper published in 1993, which measured positioning criteria on FS images following a positioning training provided by ACR, there was an incredible increase in image quality compared to the film screen images. However, still there were no categories in the new study that met the criteria 100% of the time and that is the ultimate point.
There are no perfect images every time, let alone perfection with every image.
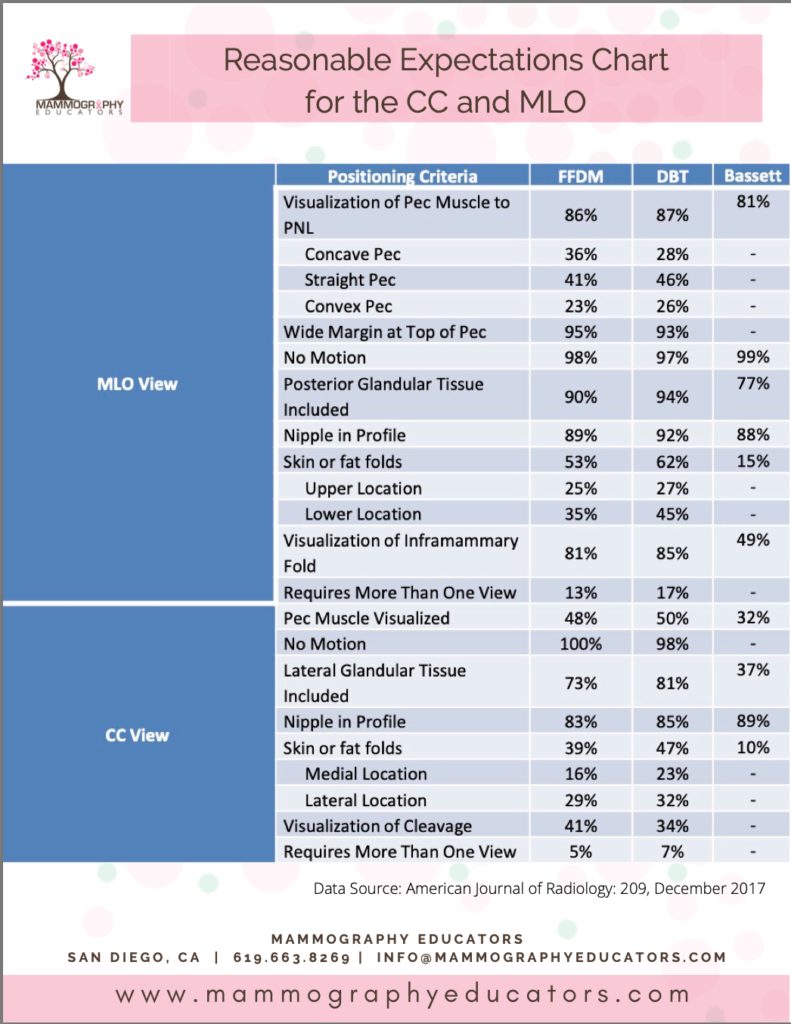
The study eventually showed us that there is an achievable level of SUCCESS:
- How often should we see the IMF on MLOs
- How often can we expect to see skin folds
- How often do we see pec on the CC
We now know. We have the data. The real beauty here is that you can use this data and information to evaluate how you are doing and what a realistic goal is. If you are not meeting these goals, there are resources to help you improve. This information can also be valuable when having conversations with your radiologists as to what IS a reasonable expectation, which is not ACR perfect.
Obviously when we submit our images for ACR Accreditation, they are supposed to be examples of our best work… so I would suggest trying to meet ALL of the criteria, but that is not everyday life. Let these percentages that are presented in this chart be used as a goalpost as to what is achievable when using proper positioning techniques.
We hope that this is helpful to you as you continue to provide the best in patient care.
